What’s a port?
When talking about Wes’ treatment, the words “port” and “access” come up all the time but it’s usually obvious that most people have no idea what we mean.
Nearly everyone is familiar with how IVs are usually performed. A needle is inserted into a vein, and then an external tube is attached that allows drugs to flow into the body through the tube and needle, and for blood to be extracted in the opposite direction. This technology is essential for medical care, but it has its drawbacks.
Some patients have veins that are harder to insert needles into than others, and this can change day to day. Changes in health, such as dehydration, can also make it more difficult. And, most significantly, the more often you need it the harder it can get – frequent insertion of needles can leave the best veins damaged, making it harder and harder to use over time. Finally, even if everything goes well, the frequency it needs to be performed is itself a problem – it be quite painful for the patient, and requires excellent technique to do, so it can be especially difficult when a patient is uncooperative or in a lot of pain. A port addresses most of these issues for patients who require frequent, long-term IV use, and as a result its common practice to install one in the first week after a leukemia diagnosis. Wes received his less than two days after diagnosis.
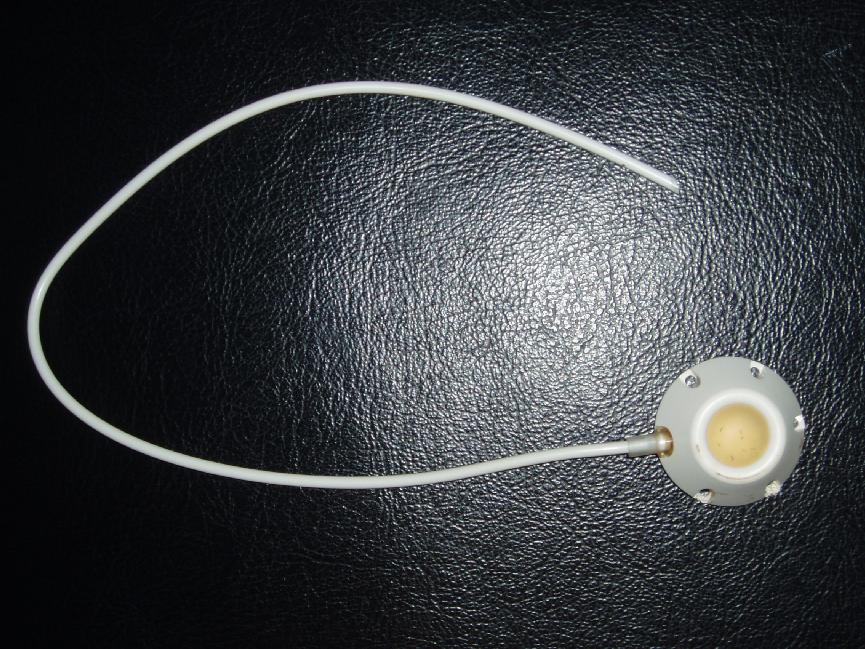
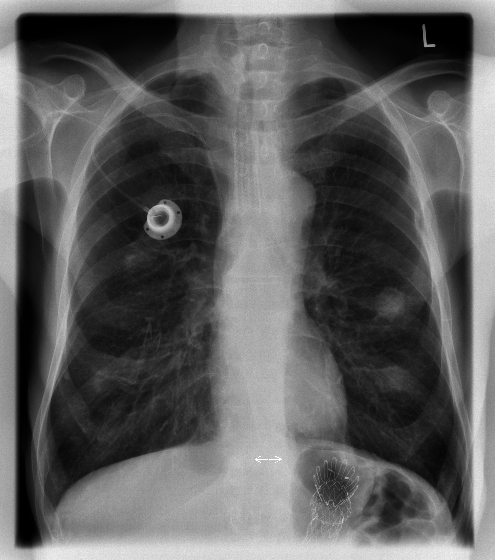
The port itself is a small device implanted under the skin, usually on the chest, consisting of two parts – the portal, and the catheter. The portal is a round device with a soft, silicone area in the middle; the portal has a plastic tube (catheter) coming out of it that is semi-permanently inserted into a vein. The surgery to install the port is relatively minor, and once installed the skin heals over it and the port is completely held inside the body, though it can be easily felt from outside.
When a patient arrives for treatment one of the first steps is to “access” the port so that it can be used. This involves poking a needle through the skin and into the port’s septum (the silicone part). Because the septum is so much larger than a vein, and just under the skin, it is much easier, quicker, and less painful than inserting a needle into a vein and requires much less practice to get it right. Once the needle is in, it is secured in place with tape and the valve at the end of the needle can be used to connect to tubes providing drugs and fluids, or to extract blood samples.
Aside from needing to be periodically flushed to ensure it remains unobstructed, a port can be left “accessed” for days or weeks at a time, significantly reducing the number of “pokes” a patient would experience. The port needs to be monitored for infection while accessed, and when a patient with a port has a fever one of the first concerns is port-site infection, but overall it is a significant improvement over the use of needles, especially for young children. When Wes is done with treatment – hopefully in 2021 – one of the last and most final steps is the procedure to remove his port.
While we’ve worked on it continually with him, Wes still doesn’t like being accessed, though it’s as much about knowing what follows the port access – chemo, in-patient stays, etc. – as the pain. Some depend on numbing cream on the port site before accessing, but in our experience this only served to increase his anxiety by giving him even more time to anticipate the access. Instead, we ask the nurses to prep out of sight as much as possible, and then it’s generally over in a minute or two.
The process itself is straightforward. We all don masks – except him, because that’s another fight – and then one of us holds him securely. His shirt is lifted up, and the nurse cleans his port-site with a disinfectant. Once clean and dry, the nurse inserts the needle assembly through his skin and into the port, makes sure it’s functioning properly, and then secures it to his chest. Finally, the nurse covers it with adhesive surgical dressing to ensure it remains sterile.
While access usually goes smoothly, it doesn’t always. This week he had one of the worst ever, leaving everyone in tears. The first attempt was with a malfunctioning needle. The second attempt went no better – the nurse couldn’t get any fluids to flow either direction. Finally, after a break to let everyone cry it out, the third attempt worked as it should. Unfortunately, de-access was almost as bad – everyone was in such a rush to get Wes home that the nurse forgot the hep-lock; he had to be accessed again just in order to properly de-access him. In case you’re keeping score at home – that’s a record four accesses in one day.
“De-accessing” is the process in reverse, but it’s much easier as Wes knows it means we are going home. First is the essential hep-lock- a saline solution is pushed into the port so that the only remaining fluid in the port is a clean solution – this helps avoid old blood clogging the port. After that, the nurse removes the dressing, pulls out the needle, and offers Wes a band-aid. That’s it. The small pinhole closes up on its own quickly almost immediately.
The videos below may be hard to watch, but it’s important for us to acknowledge what he goes through. The meltdown is all anxiety-driven, so the faster it’s over the better. What you don’t really see is how quickly he recovers – after this there is rarely any other pain involved in treatment as all blood samples can be drawn, and drugs delivered, painlessly through the port.


